




































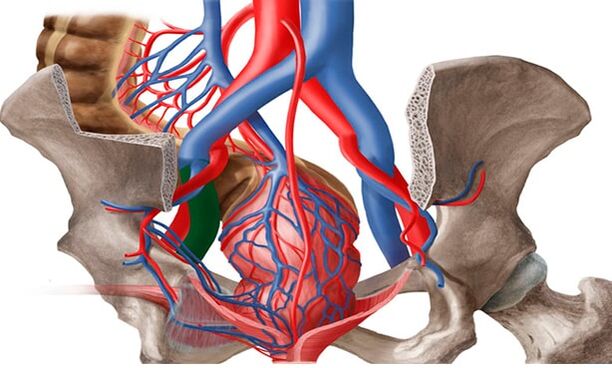
From the article you will learn the characteristics of varicose veins in women - this is a deformity of the veins of the pelvic area with reduced blood flow to the internal and external genitalia.
general information
In the literature, varicose veins are also referred to as "pelvic congestion syndrome", "varicose veins in women", "chronic pelvic pain syndrome". The prevalence of varicose veins in the small pelvis increases with age: from 19. 4% in girls under 17 to 80% in perimenopausal women. Most often, pelvic vein pathology is diagnosed in the reproductive period in patients aged 25-45 years.
In the vast majority of cases (80%), varicose vein metastasis affects the ovarian veins and is extremely rare (1%) seen in the veins of the broad ligament of the uterus. According to modern medical approaches, the treatment of VVMT should be carried out not so much from the point of view of gynecology, but, first of all, from the point of view of phlebology.
Pathology triggers
Under pelvic varicose veins in women, doctors understand a change in the structure of the vascular walls that is characteristic of other types of the disease - weakening followed by stretching and the formation of "pockets" in which blood pools. Cases that affect only the vessels of the pelvic organs are extremely rare. In about 80% of patients, along with this form, there are signs of varicose veins of the inguinal veins, vessels of the lower extremities.
The incidence of small pelvic varicose veins is more pronounced in women. This is due to anatomical and physiological features, suggesting a tendency to weaken the venous walls:
- hormonal fluctuations, including those related to the menstrual cycle and pregnancy.
- increased pressure in the small pelvis, which is characteristic of pregnancy.
- periods of more active filling of the veins with blood, including the menstrual cycles, during pregnancy, as well as during sex.
All these phenomena belong to the category of factors that cause varicose veins. And they are found exclusively in women. Most patients experience small pelvic varicose veins during pregnancy, as there is a simultaneous stratification of provocative factors. According to statistics, in men, varicose veins of the small pelvis are 7 times less common than in the fairer sex. They have a more diverse set of challenging factors:
- weakness - long-term maintenance of low physical activity.
- increased physical activity, especially lifting weights.
- portliness;
- lack of sufficient fiber in the diet.
- inflammatory processes in the organs of the urogenital system.
- sexual dysfunction or outright denial of sex.
A genetic predisposition can also lead to pathology of the plexuses located within the small pelvis. According to statistics, varicose veins of the perineum and pelvic organs are most often diagnosed in women whose relatives suffered from this condition. The first changes in them can be observed in adolescence during adolescence.
The highest risk of developing inguinal varicose veins in women with pelvic vessel disease is seen in patients with venous pathology in other parts of the body. In this case, we are talking about congenital weakness of the veins.
Etiopathogenesis
Proctologists believe that the following main reasons always contribute to the occurrence of VVP: valvular insufficiency, venous obstruction and hormonal changes.
Pelvic venous congestion syndrome can develop due to the congenital absence or insufficiency of venous valves, something that was revealed by anatomical studies in the last century and modern data confirm it.
It was also found that in 50% of patients the varicose veins are genetic in nature. FOXC2 was one of the first genes to be identified and plays a key role in the development of VVP. The relationship between disease development and gene mutations (TIE2, NOTCH3), thrombomodulin level, and growth factor-type 2 growth factor has been identified. These factors contribute to a change in the structure of the valve itself orof the venous wall - all this leads to the failure of the valve structure. dilation of the vein, which causes a change in the function of the valve. in progressive regression and eventually in varicose veins.
An important role in the development of the disease can be played by the dysplasia of the connective tissue, the morphological basis of which is the reduction of the content of different types of collagen or the violation of the ratio between them, which leads to a decrease in the strength of the veins.
The incidence of VVP is directly proportional to the amount of hormonal changes, which are particularly pronounced during pregnancy. In pregnant women the capacity of the pelvic veins increases by 60% due to the mechanical compression of the pelvic vessels by the pregnant uterus and the vasodilating effect of progesterone. This venous dilatation persists for one month after delivery and can cause venous valve insufficiency. In addition, during pregnancy, the mass of the uterus increases, changes in its position occur, which causes dilation of the ovarian veins, followed by venous congestion.
Risk factors also include endometriosis and other inflammatory diseases of the female reproductive system, estrogen therapy, adverse working conditions for pregnant women, which include hard physical work and prolonged forced posture (sitting or standing posture) during the working day.
The formation of varicose veins in the small pelvis is also facilitated by the anatomical features of the outflow from the veins of the small pelvis. The diameter of the ovarian veins is usually 3-4 mm. The long and thin ovarian vein on the left flows into the left renal vein and on the right into the inferior vena cava. Normally, the left renal vein is located in front of the aorta and behind the upper mesenteric artery. The normal angle between the aorta and the superior mesenteric artery is about 90 °.
This normal anatomical position prevents compression of the left renal vein. On average, the angle between the aorta and the upper mesenteric artery in adults is 51 ± 25 °, in children - 45, 8 ± 18, 2 ° in boys and 45, 3 ± 21, 6 ° in girls. If the angle is reduced from 39. 3 ± 4. 3 ° to 14. 5 °, aorto-mesenteric compression or nut-crushing syndrome occurs. This is the so-called anterior, or true, nutcracker syndrome, which has the greatest clinical significance. Posterior carotid artery syndrome occurs in rare cases in patients with posterior aortic or annular arrangement of the peripheral left renal vein. Obstruction of the proximal venous bed causes an increase in pressure in the renal vein, which leads to the formation of renal regression in the left ovarian vein with the development of chronic pelvic venous insufficiency.
May-Turner syndrome - compression of the left common iliac vein by the right common iliac artery - also serves as one of the causative agents of varicose veins in the pelvis. It occurs in no more than 3% of cases, it is more common in women. At present, due to the introduction of radiation and intravascular imaging methods in practice, this pathology is being identified more and more often.
Classification
Varicose veins are divided into the following forms:
- The main type of varicose veins: enlargement of the blood vessels of the pelvis. The reason is the valvular insufficiency of 2 types: acquired or congenital.
- The secondary form of pelvic vein thickening is diagnosed exclusively in the presence of gynecological pathologies (endometriosis, neoplasms, polycystic).
The varicose veins of the pelvis develop gradually. In medical practice, there are many major stages in the development of the disease. They will vary depending on the presence of complications and the spread of the disease:
- First degree. Changes in the structure of the ovarian vein valves may occur for hereditary reasons or be acquired. The disease is characterized by an increase in the diameter of the veins up to 5 mm. The left ovary has strong dilation on the outside.
- Second degree. This degree is characterized by the spread of pathology and damage to the left ovary. The veins in the uterus and right ovary may also dilate. The expansion diameter reaches 10 mm.
- Third degree. The diameter of the veins increases up to 1 cm. The dilation of the veins is observed equally in the right and left ovary. This stage is due to pathological phenomena of gynecological nature.
It is also possible to classify the disease according to the main cause of its development. There is a primary degree, in which the expansion is caused by defective function of the venous valves and a secondary degree, which is a consequence of chronic gynecological diseases, inflammatory processes or complications of oncological nature. The degree of the disease may vary depending on the anatomical feature, which indicates the location of the vascular disorder:
- Intracast a plethora.
- vulva and perineum.
- Combined forms.
Symptoms and clinical manifestations
In women, pelvic varicose veins are accompanied by severe but non-specific symptoms. Manifestations of this disease are often considered signs of gynecological disorders. The main clinical symptoms of varicose veins in the groin in women with pelvic vascular involvement are:

- Non-menstrual pains in the lower abdomen. Their intensity depends on the stage of the venous lesion and the extent of the procedure. For the 1st degree of varicose veins of the small pelvis, it is a characteristic periodic, mild pain, extending to the lower back. In later stages it is felt in the abdomen, perineum and waist and is long and intense.
- Intense mucous secretion. The so-called leukorrhea does not have an unpleasant odor, does not change color, which would indicate infection. The volume of the discharge increases in the second phase of the cycle.
- Increased symptoms of premenstrual syndrome and dysmenorrhea. Even before the onset of menstruation, the pain in women increases, until the onset of difficulty walking. During menstrual bleeding, it can become unbearable, spreading to the entire pelvic area, perineum, waist and even thighs.
- Another characteristic sign of groin varicose veins in women is discomfort during sexual intercourse. It is felt in the vagina and vagina and is characterized as dull pain. It can be observed at the end of sexual intercourse. In addition, the disease is accompanied by increased stress, irritability and mood swings.
- As with small pelvic varicose veins in men, in the female part of patients with such a diagnosis, the interest in sex gradually disappears. The cause of the dysfunction is both the constant discomfort and the reduction of the production of sex hormones. In some cases, infertility may occur.
Instrumental diagnosis
The diagnosis and treatment of varicose veins is done by a venologist, a vascular surgeon. Currently, the number of VVP detection cases has increased due to new technologies. Patients with CPP are examined at different stages.
- The first stage is a routine examination by a gynecologist: taking a souvenir, manual examination, ultrasound examination of the pelvic organs (to exclude other pathology). Based on the results, an examination is additionally prescribed by a proctologist, urologist, neurologist and other relevant specialists.
- If the diagnosis is unclear but VVPT is suspected, pelvic vein ultrasound (USAS) is performed in the second stage. This is a non-invasive, highly informative diagnostic method used in all women with suspected VVPT. If earlier it was believed that examination of only the pelvic organs was sufficient (venous examination was considered difficult to access and optional), then at this stage, pelvic vein ultrasound is a mandatory examination procedure. With the help of this method, it is possible to detect the presence of varicose veins in the small pelvis by measuring the diameters, the speed of blood flow in the veins and to find out in advance what is the main pathogenetic mechanism - failure of the ovarian veins or venous. Also, this method is used for the dynamic evaluation of the conservative and surgical treatment of VVPT.
- The examination is performed transvaginally and intra-abdominally. The peripheral veins, the inguinal plexuses, and the uterine veins are visually transvaginal. According to different authors, the diameter of the vessels of the so-called localizations ranges from 2, 0 to 5, 0 mm (on average 3, 9 ± 0, 5 mm), ie not more than 5 mm and the average diameter of the arcuate veinsis 1, 1 ± 0, 4 mm. Veins larger than 5 mm in diameter are considered dilated. The inferior vena cava, pelvic veins, left renal vein, and ovarian veins are examined intraventricularly to rule out thrombotic masses and extravascular compression. The length of the left renal vein is 6 to 10 mm and its average width is 4 to 5 mm. Normally, the left renal vein where it passes over the aorta is somewhat flattened, but a reduction in its transverse diameter of 2-2. 5 times occurs without significant acceleration of blood flow, which ensures normal outflow without increasing pressurein the predictive zone. In the case of narrowing of a vein against a background of abnormal compression, there is a significant reduction in its diameter - by 3, 5-4 times and acceleration of blood flow - over 100 cm / s. The sensitivity and specificity of this method are 78 and 100%, respectively.
- Examination of the ovarian veins is included in the mandatory examination of the pelvic veins. They are located along the anterior abdominal wall, along the rectus abdominis, slightly lateral to the iliac veins and arteries. A sign of ovarian venous insufficiency in the US is considered to be greater than 5 mm in diameter in the presence of retrograde blood flow. Ultrasound of the veins of the lower extremities, perineum, vulva, inner thigh and gluteal area should be performed for a complete examination, prevention of recurrences and proper treatment tactics.
- The development of medical technology has led to the use of new diagnostic methods. In the third stage, after the ultrasound verification of the diagnosis, diagnostic methods of radiation are used to confirm it.
- Pelvic venography with selective bilateral radiopaque ovulation is one of the invasive diagnostic methods with radiation performed only in a hospital setting. This method has long been considered the diagnostic "gold standard" for assessing dilation and detecting valvular insufficiency in pelvic veins. The essence of the method is the introduction of a contrast agent under the control of an X-ray installation through a catheter installed in one of the main veins (jugular, brachial or femoral) in the pelvic, renal and ovarian veins. Thus, it is possible to identify the anatomical variants of the structure of the ovarian veins, to determine the diameters of the gonadal and pelvic veins.
- The retrograde contrast of the gonadal veins at the height of the Valsalva test serves as a pathognomonic angiographic sign of their valvular insufficiency by visualizing a sharp dilation and torsion, respectively. This is the most accurate method for detecting May-Turner syndrome, metatrombo-venous changes in the pelvis and inferior vena cava.
- When the left renal vein is compressed, perinephric side veins are identified with retrograde blood flow to the gonadal veins, stagnation of contrast in the renal vein. The method measures the pressure gradient between the left kidney and the inferior vena cava. Normally, it is 1 mm Hg. Art. ; slope equal to 2 mm Hg. Art. , may indicate slight compression. with slope >3 mm Hg. Art. can be diagnosed with aorto-mesenteric compression syndrome with hypertension in the left renal vein and inclination >5 mm Hg. Art. is considered a hemodynamically significant stenosis of the left renal vein. Determining the pressure gradient is an important diagnostic element, since depending on its values, substantially different surgeries are planned in the veins of the small pelvis, something very important in modern conditions. Currently, this study (with a normal pressure gradient) can be used for therapeutic purposes - for ovarian vein embolization.
- The next method of irradiation is pelvic vein emission computed tomography with in vitro labeled erythrocytes. It is characterized by the deposition of labeled erythrocytes in the pelvic veins and the visualization of the gonadal veins, allows the detection of varicose veins of the pelvis and dilated veins of the ovaries in various positions, the degree of pelvic venous congestionand the perineum. Normally, the veins of the ovaries do not contrast, no accumulation of radiopharmaceutical is observed in the venous plexuses. For an objective assessment of the degree of venous congestion of the small pelvis, the coefficient of pelvic venous congestion is calculated. But this method also has disadvantages: invasiveness, relatively low spatial resolution, inability to accurately determine the diameter of the veins, therefore, is currently not used as often in clinics.
- Video laparoscopic examination is a valuable tool for evaluating the undiagnosed. In combination with other methods, it can help identify the causes of pain and prescribe the right treatment. With varicose veins of the small pelvis in the area of the ovaries, along the round and wide ligaments of the uterus, the veins can be imaged in the form of cyanotic, dilated vessels with a thin and tense wall. The use of this method is significantly limited by the following factors: the presence of retroperitoneal adipose tissue, the ability to assess varicose veins only in a limited area and the inability to determine the regression through the veins. Currently, the use of this method is diagnostically justified in cases of suspected multifocal pain. Laparoscopy can show the causes of CPP, for example, foci of endometriosis or adhesions, in 66% of cases.
Features of the treatment
For the complete treatment of varicose veins of the small pelvis, a woman must follow all the recommendations of the doctor and also change her lifestyle. First of all, you should pay attention to the loads, if they are too high, they should be reduced, if the patient follows an excessive sedentary lifestyle, it is necessary to exercise, walk more often, etc.
It is highly recommended for patients with varicose veins to adjust their diet, to consume as little junk food as possible (fried, smoked, sweet in large quantities, salty, etc. ), alcohol, caffeine. It is better to prefer vegetables and fruits, dairy products, cereals.
Also, as a precaution for the progression of the disease and for medical purposes, doctors prescribe the use of compression underwear in patients with varicose veins.
Medicines
ERCT treatment involves many important points:
- to get rid of the reverse flow of venous blood.
- relief of disease symptoms;
- stabilization of vascular tone.
- improved blood circulation to the tissues.
Preparations for varicose veins should be taken in classes. The rest of the drugs, which play the role of painkillers, are allowed to be taken exclusively during a painful attack. For effective treatment, your doctor will often prescribe the following medications:
- phleboprotectors;
- enzyme preparations?
- drugs that relieve inflammatory processes with varicose veins.
- pills to improve blood circulation.
Surgery
It is worth recognizing that conservative treatment methods give really visible results especially in the early stages of varicose veins. At the same time, the problem can be solved fundamentally and the disease can be completely eliminated only with surgery. In modern medicine, there are many variations of surgical treatment of varicose veins, consider the most common and effective types of surgery:
- embolism of veins in the ovaries.
- Sclerotherapy?
- plastic of the uterine ligaments.
- removal of dilated veins by laparoscopy.
- tightening of the veins in the small pelvis with special medical clips (clips).
- Cross-resection - vein ligation (prescribed if, in addition to the pelvic organs, the vessels of the lower extremities are also affected).
During pregnancy, only symptomatic treatment of small pelvic varicose veins is possible. We recommend wearing compression stockings, taking phlebotonics after a vascular surgeon's recommendation. In the II-III trimester, venous sclerosis of the perineal veins can occur. If, due to varicose veins, there is a high risk of bleeding during spontaneous delivery, the choice is made in favor of surgical delivery.
Physiotherapy
The physical activity system for the treatment of varicose veins in a woman consists of exercises:
- "Bike". We lie on our backs, put our hands behind our heads or place them along our body. Lifting our legs, we make circular movements with them, as if pedaling with a bicycle.
- "Birch". We sit face down on any hard, comfortable surface. Lift your legs and start gently behind your head. Supporting the lumbar region with your hands and placing your elbows on the floor, slowly straighten your legs, lifting the body upwards.
- "Pair of scissors". The starting position is on the back. Raise your closed legs slightly above floor level. Spread the lower extremities to the sides, turn them back and repeat.
Possible complications
Why are small pelvic varicose veins dangerous? The following effects of the disease are often recorded:
- inflammation of the uterus, its components.
- uterine bleeding;
- abnormalities in the work of the bladder.
- the formation of venous thrombosis (a small percentage).
Prophylaxis
In order for the varicose veins in the small pelvis to disappear as soon as possible and in the future to prevent recurrence of the pathology of the pelvic organs, it is worth following simple precautionary rules:
- perform gymnastic exercises daily.
- prevention of constipation;
- follow a diet that should be high in fiber.
- do not stay in one place for a long time.
- take a contrast shower of the perineum.
- to prevent varicose veins, it is best to wear extremely comfortable shoes and clothes.
Preventive measures aimed at reducing the risk of the appearance and development of varicose veins in the small pelvis are mainly limited to the normalization of lifestyle.